NEWS: NT Study Quantifies Hospital Cost of Housing Failure – $72 Million Annually
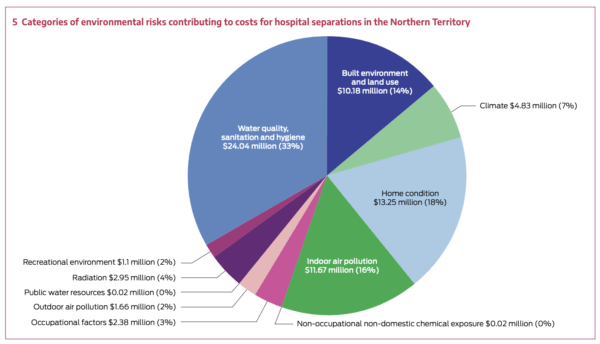
A Medical Journal of Australia study has put a dollar figure on the well established fact: poor housing makes people sick, and fixing it saves money. Environmental risk factors—primarily water quality, sanitation, and home condition—cost Northern Territory public hospitals $72 million in a single year.
The retrospective analysis of 174,194 hospital admissions between July 2021 and June 2022 found that 12,150 separations were directly attributable to preventable environmental risks. These weren’t inevitable hospitalisations. They were the measurable consequence of infrastructure failure.
The Health Hardware Cost
Two categories dominated the $72 million burden: “water quality, sanitation and hygiene” contributed over $24 million, while “home condition” added $13 million. Together, these health hardware failures accounted for more than half the total environmental cost—$37.3 million that could have been prevented through functional taps, showers, washing machines, toilets, and drainage.
Skin infections represented the largest single disease cost at $26.4 million. These weren’t minor presentations. The category included cellulitis, abscesses, pustules and impetigo, conditions that progress to acute rheumatic fever and rheumatic heart disease when housing infrastructure fails to support basic hygiene.
Lower respiratory tract infections added $13.1 million, cardiac disease $9.8 million. Each diagnosis linked back to environmental conditions: overcrowding, poor ventilation, dysfunctional washing facilities, inadequate drainage.
Who Bears the Cost
Indigenous Territorians, who represent 30% of the NT population, accounted for 65% of environmentally attributable hospital costs: $47.2 million compared with $24.8 million for non-Indigenous people. Remote areas bore $41.7 million of the total burden. Children aged 0-4 years accounted for $10.9 million in costs.
These disparities don’t reflect behaviour. They reflect systemic infrastructure inequality.
The Underestimate
The $72 million figure captures inpatient hospital separations only. It excludes outpatient appointments, emergency department presentations, primary care visits, community health services, and the health workforce costs of managing preventable disease. The true economic burden is substantially higher.
The study’s authors explicitly recommend “targeted interventions to reduce inequities in housing, sanitation and water quality” and cite Housing for Health evidence from NSW showing 40% reductions in infectious disease hospitalisations after systematic housing improvements.
The Northern Territory now has more quantified evidence that health hardware maintenance is cost-effective health infrastructure. The question is whether government investment will match the scale of preventable harm the data reveals.